
Introduction
Patent foramen ovale (PFO) is a very popular topic in scuba diving as the appreciation of its relationship to decompression sickness (DCS) becomes more widespread in the diving community. Though the incidence of DCS in recreational diving is only about 2 episodes per 10,000 dives, decompression sickness affects approximately 1000 divers per year. The presence of a PFO is felt to increase the risk 5- to 13-fold (1-3). An understanding of the link between PFO and DCS as well as various treatment options is important to all divers.
Incidence and Anatomy
The patent foramen ovale is an integral part of the normal fetal circulation. The inferior vena cava is the large vein in the abdomen that delivers deoxygenated blood from the abdomen and lower extremities to the right atrium. The placental oxygenated blood from the mother empties into the inferior vena cava of the fetus. Normally, a portion of the blood from the inferior vena cava passes from the right atrium to the left atrium through the PFO during fetal life, bypassing the fetal lungs as they are collapsed and full of fluid. At birth, the lungs expand and are used to oxygenate blood for the baby. The pulmonary blood flow increases greatly, increasing left atrial pressure. The resulting atrial pressure differences compress the septum primum against the septum secundum, functionally closing the PFO. Anatomic closure of the PFO occurs later in infancy in most people but is

incomplete in approximately 25% of the population (4-5), leaving these individuals at risk for right to left shunting (blood continues to flow from the right side of the heart to the left side).
PFO diameters are quite variable in size ranging from 1-19 mm with the average size being larger in older adults (4), suggesting PFOs may continue to enlarge during life.
Relationship of PFO to DCS
It was first suggested in 1986 that a cardiac right to left shunt may be important for paradoxical gas embolism (venous bubbles going from the right side of the heart to the left side of the heart) in scuba divers (13). Subsequently, the importance of PFO for DCS in divers has been further investigated (1, 7-10). As mentioned above, the risk of DCS in sport divers is quite low but is increased by at least 5-fold in the presence of a PFO (1-3). Additionally, the average number of ischemic brain lesions as seen on MRI in experienced divers with PFO has been reported to be twice as high as in divers without PFO (11). The cause and clinical significance of these findings are unclear, but they might suggest small, unnoticed air bubbles passing through the small opening in the heart (PFO) and reaching other parts of the body.
There are four types of decompression sickness felt to be associated with PFO. These are cerebral (stroke-like), spinal (paralysis), inner ear (vertigo), and cutaneous (skin bends). Of note, pain only decompression sickness is not felt to be associated with PFO. If a PFO is found in this case, it should be considered an “innocent bystander” and closure is not warranted.
Diagnosis
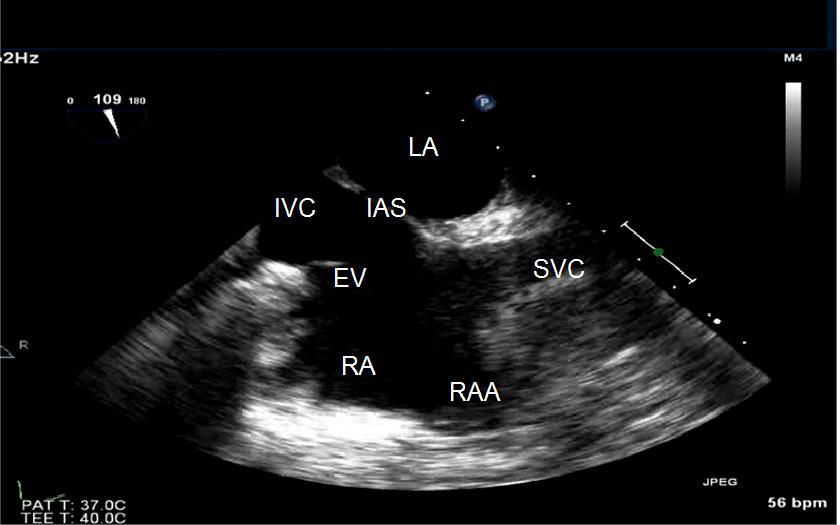
Two types of heart ultrasounds are used to diagnose a PFO: transthoracic echocardiography (TTE), a non-invasive external ultrasound, and transesophageal echocardiography (TEE), a more detailed test performed with a probe inserted down the throat. TTE is the preferred diagnostic test of choice, given its less invasive nature. TEE, while more invasive, gives better visualization of the atrial septum resulting in greater sensitivity in making the diagnosis. As a result, TEE is usually reserved for divers where there is a very high index of suspicion for PFO but the TTE was inconclusive.
A bubble study is where two syringes of normal saline solution are flushed back and forth into each other via a stopcock to produce very small bubbles in the solution (called “agitated saline”) and then this solution is injected into an arm vein of the subject. A bubble study increases the diagnostic sensitivity of a PFO by enhancing echocardiographic detection of the intermittent right-to-left shunting across a typical PFO and should always be performed in divers when PFO is a concern. Agitated saline contrast injected intravenously during Valsalva maneuver with release of straining when contrast is visualized in the right atrium increases sensitivity. When microbubbles are seen moving directly from the right atrium to the left atrium during the test, it confirms that there is an opening between the two chambers of the heart (a PFO). However, in some cases, the exact pathway of the bubbles may not be clear due to technical challenges. If bubbles show up in the left atrium right after appearing in the right atrium, it strongly suggests a PFO. On the other hand, if the bubbles take longer—more than five heartbeats—to reach the left atrium, it may indicate other conditions, like abnormal connections between the lungs and the left atrium.
If the contrast bubbles are injected into a vein in the arm, they can sometimes get mixed with bubble-free blood flowing from the inferior vena cava (a different vein), which might hide the PFO and give a false negative result. Using the femoral vein for the injection can improve detection because it directs the bubbles more accurately toward the suspected opening. However, inserting an IV in the groin is often not practical for routine testing.
Therapeutic Options
No specific guidelines exist for PFO closure in people who have decompression illness, but the options are to stop scuba diving, decrease the depth and/or time of dives to limit the inert gas load, or undergo percutaneous PFO closure. Some divers decide that they have many other interests and diving is not that important to them. These divers will frequently give up the sport. Other divers who enjoy the sport but dive infrequently often opt for diving “conservatively” to limit their bubble-load. This would involve no-decompression diving, limiting depths to less than 100 feet (30 meters), diving nitrox on air profiles, prolonged (more than the usually recommended 3-5 min) safety stops at approximately 15-20 feet (5-6 meters) at the end of their dives, and limiting the number of dives per day to one or two.
People who make their living through scuba diving (instructors, divemasters, etc) and divers who enjoy more aggressive types of diving such as deep wrecks, cave diving, rebreather diving, and mixed gas diving often elect percutaneous closure of the PFO. This also holds true for divers who have had recurrent “unexpected” DCS events despite diving conservatively as defined above.
Treatment Results
A 2012 study reported the results of conservative diving practices after an episode of DCS (14). Eighteen divers in this study had a right-to-left shunt, nine were small and nine were large. Mean follow-up was 5.3 years (range 0-11 years). Four of these divers had undergone PFO closure and had no episodes of DCS in follow-up. The absolute risk of suffering DCS before examination for the remaining 14 divers with right-to-left shunt and no closure was 23.5 DCS events per 10,000 dives for those with a small shunt compared to 71.6 for those with a large shunt. After recommendation for conservative diving practices, the DCS risk at follow-up fell to 6.0 per 10,000 dives in the small shunt group and zero in divers with the large shunt. The major limitation to this study is its small sample size, but the results suggest a need for more studies of conservative diving practices for divers with right to left shunts.
When DCS has occurred, especially after so called “undeserved” cases of DCS, divers are often encouraged to seek screening for a shunt and some diving medical societies classify these divers as ineligible to return to diving (22). There are also several diving medical specialists who recommend divers with a history of DCS and a positive right-to-left shunt to undergo closure if it turns out to be a PFO, even though there is no clear evidence to indicate that this intervention reduces the risk of DCS or neurologic events (16-19).
However, in a 2011 study of 83 scuba divers with a history of DCS and a follow-up of 5.3 years, 28 divers had no PFO, 25 had a PFO closure, and 30 continued diving with a PFO without closure (20). At the beginning of the study, there were no significant differences between the groups in the number of dives, dive profiles, diving depth, or cumulative dives to more than 40 meters of salt water (msw). After follow-up, while there were no differences between the groups with respect to minor DCS events, the risk for major DCS was significantly higher in the divers with PFO and no closure than in divers with PFO and closure or divers without PFO. Although this offers new evidence that PFO closure reduces the risk for major DCS, the authors do not recommend closure in all divers with a history of DCS but rather recommend further studies to confirm these results.
Percutaneous PFO Closure
The closure procedure for a patent foramen ovale is relatively painless and is done percutaneously using a needle stick – not surgery – through a femoral vein in the groin. Imaging during the procedure is done with a combination of fluoroscopy (x-ray) and ultrasound imaging, either TEE or intracardiac echo. The most common device in use in the United States is the Amplatzer PFO Occluder. This is a wire mesh made out of nickel and a titanium alloy. The device is filled with securely sewn polyester fabric to help close the defect. It is deployed through a small catheter which has been placed across the PFO. The procedure takes about an hour and patients are usually discharged home the same day or the following morning.

Amplatzer PFO Occluder: Used to close the defect
Conclusions and Recommendations
Should all divers be screened for a PFO?
No. There is approximately a 5-fold increased relative-risk of DCS in patients with PFO, but the absolute risk is still quite small.
Should all divers with DCS be screened for a PFO?
No. Twenty five percent of the population has a PFO so one would expect a similar percentage of divers with DCS to have a PFO. Not all scuba dives have the same risk of DCS. To paraphrase James Carville’s famous quote from the first Clinton presidential campaign, “it’s the bubble, stupid”. The issue with decompression sickness is the inert gas “bubble load”, not the PFO. However, episodes of DCS in “low-risk” dives, especially neurologic events, or multiple “undeserved” DCS events should prompt investigation for PFO.
Should all divers with DCS and PFO have a PFO closure?
No. Options for divers with PFO and DCS include discontinuing diving, conservative diving practices, or PFO closure. Recommendations should be made on a case-by-case basis based on the DCS event(s), the type of diving being performed by the diver involved, and the risks of PFO closure.
References:
Wilmshurst, PT, Byrne JC, Webb-Peploe MM. Relation between interatrial shunts
and decompression sickness in divers. Lancet. 1989;334:1302-1306
Torti SR, Billinger M, Schwerzmann M. Risk of decompression illness among 230
divers in relation to the presence and size of patent foramen ovale. Eur Heart J
2004;25:1014-1020
Bove AA. Risk of decompression sickness with patent foramen ovale. Undersea
Hyperb Med 1998;25:175-8.
Hagan PT, Scholz DG, Edwards WD. Incidence and size of patent foramen ovale
during the first 10 decades of life: an autopsy study of 965 normal hearts. Mayo
Clin Proc 1984;59:17-20.
Kerut EK, Norfleet WT, Plotnick GD, Giles TD. Patent foramen ovale: a review of
associated conditions and the impact of physiological size. J Am Coll Cardiol
2001;38 (3): 613-623.
Wilmhurst PK, Ellis BG, Jenkins BS. Paradoxical gas embolism in a scuba diver
with an atrial septal defect. Br Med J (Clin Res Ed) 1986;293:1277
Moon RE, Camporesi EM, Kisslo JA. Patent foramen ovale and decompression
sickness in divers. Lancet 1989;1:513-14.
Germonpre P, Dendale P, Unger P, et al. Patent foramen ovale and
decompression sickness in sport divers. J Appl Physiol 1998;84:1622-6.
Germonpre P, Hastir F, Dendale P, et al. Evidence for increasing patency of the
patent foramen ovale in divers. Am J Cardiol 2005;95;912-15.
Gempp E, Blattearu J, Stephant E, et al. Relation between right-to-left shunts
and spinal cord decompression sickness in divers. Int J Sports Med 2009;30:150-3.
Schwerzmann M, Seiler C, LippE, et al. Relation between directly detected
patent foramen ovale and ischemic brain lesions in sport divers. Ann Intern Med
2001:134:21-4.
Schuchlenz HW, Weihs W, Hackl E, Rehak P. A large Eustachian valve is a
confounder of contrast but not of color Doppler transesophageal
echocardiography in detecting a right-to-left shunt across a patent foramen ovale.
Int J Cardiol 2006;109:375-80.
Gin KG, Huckell VF, Pollick C. Femoral vein delivery of contrast medium
enhances transthoracic echocardiographic detection of patent foramen ovale. J
Am Coll Cardiol 1993;22:1994-2000.
Klingmann, C, Rathmann N, Hausmann D, et al. Lower risk of decompression
sickness after recommendation of conservative decompression practices in
divers with and without vascular right-to-left shunt. Diving and Hyperbaric
Medicine 2012;42(3):146-150.
[Swiss Underwater and Hyperbaric Medical Society. Empfehlungen 2007. Der
Schwiezerischen Gesellschaft Fur Unterwasser-und Hyperbarmedizin Zum
Tauchen Mit Einem Offenen Foramen Ovale][cited 2012 June11]. Available from:
Scott P, Wilson N, Veldtman G. Fracture of a GORE HELEX septal occluder
following PFO closure in a diver. Catheter Cardiovasc Interv 2009;73:828-31.
Wahl A, Praz F, Stinimann J, Windecker S, Seiler C, Nedeltchev K, et al. Safety
and feasibility of percutaneous closure of patent foramen ovale without intra-
procedural echocardiography in 825 patients. Swiss Med Wkly. 2008:138:567-72.
Saguner AM, Wahl A, Praz F, et al. Figulla PFO occlude versus Amplatzer PFO
occlude for percutaneous closure of patent foramen ovale. Catheter Cardiovasc
Interv 2011;77:709-14
Furlan AJ, ReismanM, Massaro J, et al. Closure or medical therapy for
cryptogenic stroke with patent foramen ovale. N Engl J Med. 2012;366:991-9.
Billinger M, Zbinden R, Mordasini R, et al. Patent foramen ovale closure in
recreational divers: effect on decompression illness and ischaemic brain lesions
during long-term follow-up. Heart. 2011;97:1932-7.

Douglas Ebersole, MD is an interventional cardiologist at Watson Clinic in Lakeland, Florida as well as the Director of the Structural Heart program at Lakeland Regional Health medical center. He is an avid technical and cave diver as well as a CCR trimix instructor and cardiology consultant to Divers Alert Network (DAN). His medical background and diving experience gives him a unique perspective on diving physiology.